
It is important to understand the anatomy — mainly the myofascial structures and other possible pain generators such as nerves and intervertebral discs that relate to the abdominal and lower back area — before we start talking about certain injuries, most common causes, and treatments. It is also important to make the necessary distinction between a muscle and fascia.
Most people are familiar with what a muscle is, what it looks like and what it does. However, many people are not familiar with fascia. Even among health-care providers, fascia is not well understood yet. Fortunately with more recent emerging evidence — most importantly the work of the Stecco family out of Padova, Italy — we now understand and know more about fascia and myofascial units than we ever did before.
What Is Fascia?
Fascia can be thought of as a spider web / gluey fabric that holds us together. It connects every structure (muscles, adipose tissue, organs, arteries, veins, nerves, bones, ligaments, tendons, etc.) creating a structural continuity that gives form and function to every tissue and organ. More technically, it is a three-dimensional, soft, collagen-containing, loose and dense fibrous connective tissue that permeates the whole body.
Between its layers, fascia has loose fiber tissue that allows it to glide. One of the main substances enabling this gliding motion is a glycosaminoglycan called hyaluronic acid. This system of fibrous connective tissues influences one another throughout the entire body — meaning a dysfunction in the fascia of the foot can have an effect far from its actual site. A helpful analogy is a t-shirt being pulled from one direction and how that affects the shape of the entire shirt.
Fascia is also highly innervated with receptors that mediate proprioception and pain — playing a crucial role in many neuromusculoskeletal injury presentations.
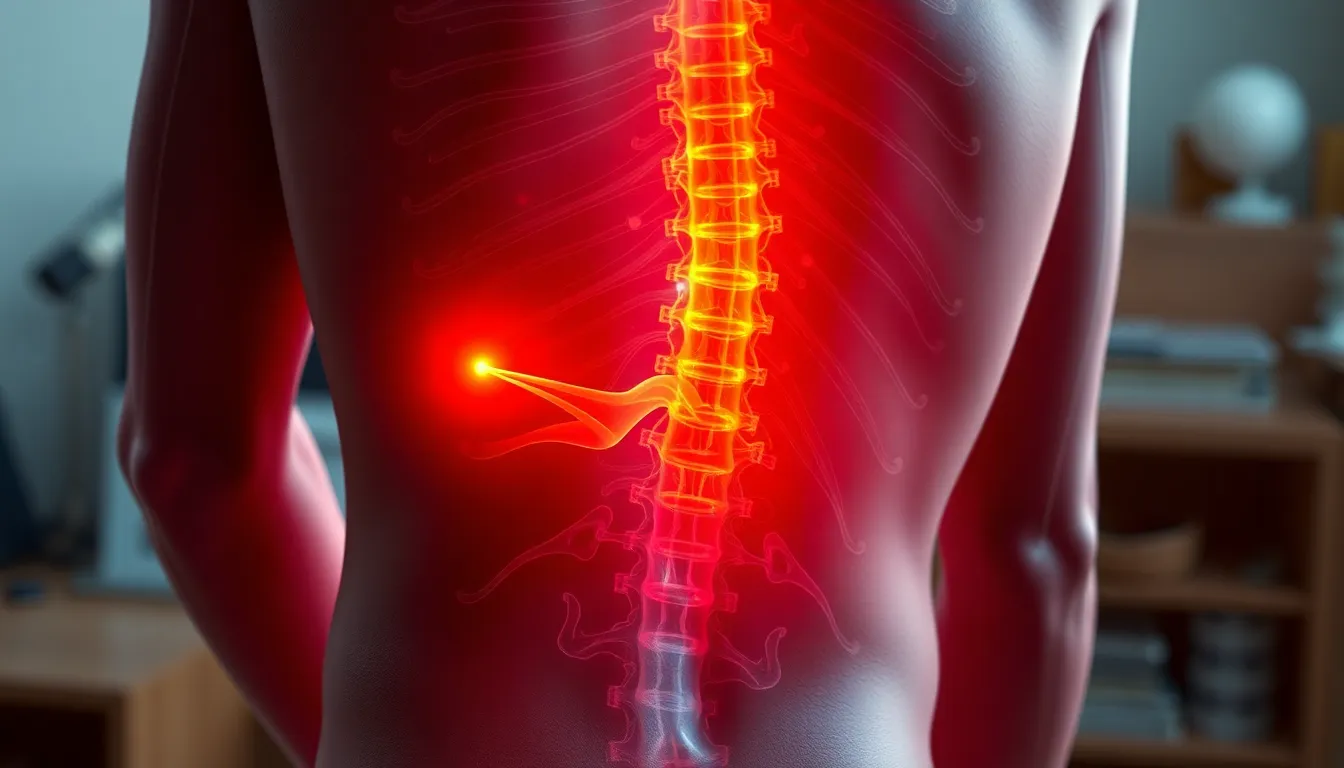
Anatomy of the Lower Back
The lumbar, sacral, and coccygeal segments make up the “lower back.” The lumbar spine is made up of 5 vertebrae (L1–L5). Between each vertebra is an intervertebral disc that absorbs shock and creates space at the neural foramen for the nerve roots (L1–S1) to exit. The spinal cord runs through the spinal canal and gives off the nerve roots that travel to their innervated tissues.
Superficial fascial structures of the lower back:
- Rectus Sheath (covering rectus abdominis)
- Deep Abdominal Fascia (covering external oblique)
- Deep Fascia of the Back (covering latissimus dorsi and lower trapezius)
- Thoracolumbar Fascia (covering the lower back area)
- Gluteal Fascia (covering the gluteal muscles)
Superficial musculature: Rectus Abdominis, External Oblique, Latissimus Dorsi.
Deeper musculature: Internal Oblique, Quadratus Lumborum, Iliocostalis Lumborum, Longissimus Thoracis, Serratus Posterior.
Deepest stabilizers: Psoas Major, Psoas Minor, Multifidus, Interspinales, Intertransversarii. Frequently we see dysfunction in these deep stabilizers — most commonly the multifidi.
Prevalence and Common Causes
According to the World Health Organization, lower back pain is the most common musculoskeletal disorder in the world, with a prevalence of ~568 million people. According to the NIH, at least 80% of Americans will experience lower back pain in their lifetime.
Acute pain lasts a few days to a few weeks. Chronic pain continues for 12 weeks or longer. Most cases are mechanical — the dysfunction lies within muscles, nerves, the spine, or the intervertebral discs.
Common acquired causes include traumatic injuries, fractures, sprain/strain, discogenic pain, myofascial pain, degeneration, and spinal stenosis. In most cases there is either mechanical pressure (from disc material, bony protrusions, or fascial compression) or chemical irritation that inflames a nerve root or peripheral nerve — producing numbness, tingling, or burning that can travel down the lower extremity.
Self-Care: Things You Can Do Today
Good news: most lower back pain resolves on its own even without clinical care. If you’re currently experiencing an episode, here are several things you can do.
- Notice how and when it started.Lower back pain rarely happens overnight — it’s usually accumulated insult. “The straw that broke the camel’s back” is a good analogy.
- Identify what makes it worse. Avoiding aggravators speeds healing — think of how picking a scab keeps reopening the wound.
- Identify what makes it better.Doing more of what doesn’t aggravate accelerates recovery.
- Ice or heat? Ice constricts blood flow and may delay needed inflammation; heat may add excess inflammation. We usually recommend movement instead — even a 15–20 minute pain-free walk every day can go a long way.
Find Your Directional Preference (McKenzie)
Frequently, flexion movements (sitting, bending forward, going up stairs) aggravate lower back symptoms while extension (lying on your stomach, the cobra pose) relieves them. But it is essential to find your directional preference.
Flexion test: Standing with feet together, bend down toward your toes and return to neutral. Repeat ~20 times. Note whether symptoms improve or worsen.
Extension test: Lie on your stomach. Place hands beneath your shoulders and press up as far as comfortable, then return, keeping the lower extremities and glutes relaxed. Repeat ~20 times and note your symptoms.
Once you identify your directional preference, perform that exercise 20 reps every 2–3 hours for ~2 weeks while avoiding the opposite direction as much as possible.
Watch the Location of Your Symptoms
The further your symptoms travel from the spine, the worse the insult — the closer they are, the better. Symptoms moving from leg back into the lower back can indicate improvement (centralization). Increasing leg symptoms while back pain disappears can indicate a sequestrated disc — seek help immediately.
If you have lower extremity symptoms (back of thigh, leg, foot, or front of thigh), try this: lie on your couch on the side opposite your symptoms, bring your knees to your chest, and let them dangle off the couch. This opens the neural foramen and decompresses the inflamed nerve.
Nutrition That Supports Healing
- Increase protein, omega-3 fats, and overall calorie intake to support tissue repair.
- Emphasize nutrient-dense vegetables.
- Avoid processed foods, trans fats, refined sugar, and refined carbohydrates.
- Some patients are sensitive to caffeine, which can tighten the lower back.
- Favor cooking methods that minimize advanced glycation end-products (AGEs) — boiling, poaching — over broiling or grilling.
- Consider thorough blood work to identify deficiencies that may contribute to neuromusculoskeletal symptoms.
- Always check the side effects of medications and supplements you’re taking.
Red Flags — Seek Help Immediately
Change in bowel or bladder function, loss of balance, muscle atrophy, or change/loss of sensation around the genital area can indicate cauda equina syndrome — a serious emergency.
What Should Clinical Treatment Look Like?
A complete treatment plan addresses every component above: understanding pain generators, identifying directional preference, assessing and treating myofascial components, identifying and treating involved nerves, optimizing diet and nutraceutical intake, correcting biomechanical issues, and resetting the brain’s perception of pain through neuromuscular re-education. By the end of care you should understand your situation, how to prevent recurrence, what to do if it returns, and when to seek further care.
Our Approach at Functional Restoration Institute
Excellent clinical care comes from an even better assessment process. Your initial visit (about 90 minutes) includes a thorough medical history, comprehensive neurological, orthopedic and chiropractic exam, review of any imaging or labs, and a conservative trial treatment.
Every follow-up begins with an in-depth conversation about your progress, followed by a treatment designed specifically for you (about 30–45 minutes). Treatments are guided by the most up-to-date research in pain science, fascia therapy, neurodynamics, and neuromuscular rehabilitation — combined with our clinical experience. We do not believe in “cookie-cutter” medicine.